Sixteen million people in the United States have type-2 diabetes, which
shortens lifespan by up to 15 years, leads to almost 300,000 deaths
annually, and costs about $100 billion annually. Since 1980 the incidence
has increased by
30%. Born in the year 2000, your male child’s lifetime risk of
developing type-2 diabetes is nearly 33%, and a female’s risk will be 39%
when following the Western diet.1 Worldwide, 135 million people have
type-2 diabetes and by 2025 the incidence is predicted to reach 300
million people worldwide.
This form of diabetes was once referred to as “adult-type diabetes”
because in the past, type-2 diabetes was rare in children. However, over
the last two decades, there has been a 10-fold increase in incidence of
type-2 diabetes in children, because of the rapidly growing numbers with
obesity from an escalating exposure to rich foods, compounded by a lack of
exercise.2
The general state of poor health of Westerners, as reflected by
diabetes, escalates unchecked for 3 important reasons:
1) This growing epidemic of type-2 diabetes and obesity is fueled by
huge profits generated by a food industry super-sizing everything by
stuffing their irresistible morsels with fat, sugar, refined flour, and
calories.
2) Medical doctors continue to prescribe remedies that have never cured
a single case of diabetes. Furthermore, the usual “poly-pharmacology” of
medications they rely upon promotes weight gain, heart disease, and
hypoglycemia, along with other serious adverse effects. From all these
expensive medications there is a small reduction in complications, such as
kidney and eye damage, which still fails to offset the tremendous harm
done by their efforts.
3) The American Dietetic Association has remained steadfast in their
recommendation of a portion-controlled version of the Western (American)
diet – an impossible diet to follow (because of its complex rules and
semi-starvation nature) – made up of ingredients, like fat, sugars,
refined foods, and cholesterol, that caused the patients’ problems in the
first place.
In 1927 Dr. E. P. Joslin, founder of the famous Joslin Diabetic Center
in Boston, suspected a high-fat, high-cholesterol diet might favor the
development of diabetes and its major complication, atherosclerosis.3 He
prophetically wrote: “I believe the chief cause of premature
atherosclerosis in diabetes, save for advancing age, is an excess of fat,
an excess of fat in the body (obesity), an excess of fat in the diet, and
an excess of fat in the blood. With an excess of fat diabetes begins and
from an excess of fat diabetics die, formerly of coma, recently of
atherosclerosis.” And now, 75 years after Joslin’s farsighted message,
diabetes is the fastest growing disease in the world.
Diabetes Is an Adaptive Response to Over-nutrition
The malnutrition caused by the high-fat, low-fiber Western diet places
serious burdens on the body and requires it to make adaptions in order to
survive under adverse conditions. The calories consumed in excess of our
needs cause us to gain fat – this is a natural, expected change. Soon a
point is reached when this accumulation becomes counterproductive – a
point when any further excess body weight is likely to cause serious
physical harm. When this hazardous excess is reached, the body puts “the
brakes on” in order to slow the rate of gain. This is accomplished by a
variety of changes that cause the hormone insulin to become less potent.
13,14 In other words, our cells become resistant to the actions of the
fat-gaining hormone, insulin – a state referred to as “insulin
resistance.”
One of insulin’s primary jobs is to push fat into the fat cells – thus
saving fat for the day when no food is available (which for Westerners
never comes). If it were not for the adaptive mechanisms which allow for
the development of “insulin resistance,” people would commonly expand
until they became so large that they could not get out of bed or fit
through a doorway – a very rare condition that does occur in 1000-pound
sized people who need a forklift to move them to the hospital. (They make
headlines in the newspaper.)
One of insulin’s other important jobs is to let sugar into the body’s
cells – with a state of “insulin resistance” the sugar cannot get into the
cells easily – so it rises in the blood. The hallmark of the diagnosis of
diabetes is an elevated blood sugar above normal (usually normal is below
115 mg/dl fasting). With impotent insulin, the calories of fat and sugar
we consume cannot easily enter the cells; the body is essentially starving
itself from the inside in a desperate attempt to compensate for the
overfeeding coming from the outside. To further reduce the burden of
obesity, the body eliminates calories by allowing sugar to spill over into
the urine, like water falling over a dam. At this stage sugar is found
with a urine test – another common way to diagnosis diabetes. Most doctors
and patients view the elevated blood sugar as the enemy to be beaten down
with medications – the result is a fat, sickly patient with a slightly
lower blood sugar.
The Reason Medical Therapy Should Be Your Last Choice
Diabetic medications have never cured anyone of diabetes and actually
compound the patients’ problems. The patient goes to the doctor, is
diagnosed with diabetes, placed on medication, and told to lose weight.
Unfortunately, these medications make insulin more effective, causing more
fat to be stored in the fat cells. The average initial weight gain when
diabetic medications are started is 8 to 20 pounds – due to partially
counteracting the protective effects of “insulin resistance.” Thus the
well-behaved patient takes the medications as directed, but then gains
weight, and as a result of the added weight his diabetes becomes worse.
The patient returns to the doctor, is given a firm scolding for gaining
weight, and then more medications are prescribed because his sugars are
even higher than before – this additional medication makes the patient
even fatter and the diabetes more out of control. The vicious cycle
continues – and the patient and doctor are left guilt-ridden and confused
about their obvious medical failure. After all, they followed the
pharmaceutical company’s instructions exactly. Worse yet, the patients are
not one bit healthier from all this effort and expense.
More than 30 years ago, when I was in medical school, I remember
doctors arguing about the benefits from aggressive use of medication to
make the blood sugars lower, a practice referred to as “tight control.”
Ideally, keeping the blood sugars close to normal makes sense, but in real
life more harm than good is done for type-2 diabetics. First of all, no
matter how hard the patient and the doctor work at their goal, the blood
sugar readings are all over the place – one test shows 60 mg/dl and the
next 260 mg/dl. Soon it becomes obvious to the patient that the short-term
goal of “normalizing” the blood sugar levels is impossible using
medications.
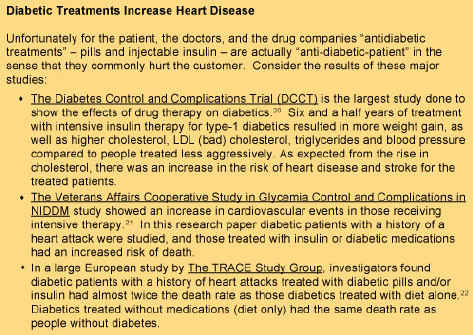
The next carrot held out is for long-term benefits: preventing
complications later in life. In truth, studies have shown there is some
benefit for the eyes and the kidneys with better control of blood sugar
(especially for type-1 diabetics).15-17 However, the major threat to the
life of a diabetic is from heart attacks and strokes – diseases of the
large blood vessels. Intensive medical therapy using the most high-tech
drugs to lower blood sugars has failed to reduce the risk for, and improve
survival from, these two major killers. In fact, the medications used to
combat sugar will actually create more sickness and death from heart
disease.
Since the early 1970s every single edition of the Physician’s Desk
Reference, found in every doctor’s office, has carried this warning in
heavy back print for their diabetic medications: “SPECIAL WARNING ON
INCREASED RISK OF CARDIOVASCULAR MORTALITY.” The most commonly prescribed
diabetic medications, known as sulfonylureas,* cause fundamental changes
in the function of cells that increase the risk of heart attacks.18 These
drugs, which are called “antidiabetic agents” by the pharmaceutical
companies, have recently been shown to more than double the risk of heart
attacks and almost triple the risk of early death in patients after an
angioplasty.19 I never prescribe this type of diabetic pills, and always
ask my patients to stop them. All diabetics should be actively looking for
a better approach – and so should any doctor interested in his patients’
welfare.
The Treatment of Type-2 Diabetes with a Low-Fat, Plant-Food Diet
Multiple studies dating as far back as the 1920s have shown the
benefits of a high-carbohydrate, low-fat diet in the treatment of type-2
diabetes.23 For example, studies from the University of Kentucky Medical
School reported as many as two-thirds of diabetics were able to
discontinue insulin and almost all stopped oral agents.24 A recent
thorough review of the use of a vegetarian diet in the treatment of type-2
diabetes was published in the September 2003 issue of the American Journal
of Clinical Nutrition. In this review article Dr. David Jenkins reported
on research showing improvements in blood sugars in diabetics with 39%
stopping insulin and 71% stopping diabetic pills after three weeks of
therapy.25 Relief of diabetic neuropathy pains, reduced lipids
(cholesterol and triglycerides), and weight loss have also been reported
with a low-fat, pure-vegetarian diet. Another recent research paper has
reported similar findings with a low-fat vegetarian diet.26 Many of these
people with type-2 diabetes are cured of their disease within three weeks,
and most will be cured of their diabetes over time as they adhere to a
low-fat, high carbohydrate diet, exercise, and lose all of their excess
body fat.
This same kind of diet (in large part because of the restriction of
animal protein) has been shown to dramatically improve the health of the
kidneys of diabetics (protein in the urine, a sign of diabetic kidney
damage, decreases and disappears).27,28 Research has also shown diabetic
damage found in the eyes (retinopathy) can be reversed with a low-fat
diet.29,30 It’s interesting how kidney and eye damage, the two purported
benefits from drug therapy, are actually better treated with diet than
with medications, at no cost and no side effects. A low-fat vegetarian
diet has also been shown to reverse heart disease (atherosclerosis), the
number one killer of diabetics.31 Many other researchers have praised a
low-fat vegetarian diet as the best approach to prevent and treat most
diseases that plague people in modern societies, including people with
diabetes.32-35 Possibly the most important effect of this dietary approach
(combined with exercise) is the scientifically established fact that this
is the easiest and most effective way to lose weight permanently.36-39
Obesity is the underlying cause of diabetes.40
Practical Steps to Cure Type-2 Diabetes
If you are one of the millions of diabetic patients facing a hopeless
future of worsening diabetes, obesity, loss of vision, kidney failure,
heart attacks, strokes, gangrene, and early death and disability – even
though you have visited your doctors regularly, and taken your medications
faithfully – then it is time to break this downhill spiral by changing
your diet and exercise program. At the same time ask your doctor to
provide you with sensible, conservative, care. I do the following with my
patients:
1) Stop diabetic pills and reduce or eliminate insulin. In most cases,
I have my patients stop all of their diabetic pills the day they start the
McDougall diet and exercise program and/or at least half of their insulin.
If this reduction is not made in a timely manner, then they run a real
risk of developing hypoglycemia (too low blood sugar). I increase or
reduce medications based on the patient’s response and as a general
guideline I try to keep their blood sugars between 150 to 250 mg/dl while
I am trying to adjust their medication needs. Stopping and/or reducing the
medications reverses the weight gain immediately. (Insulin cannot be
stopped in type-1 diabetes, but the dosage is often reduced.)
2) Change them to a low-fat, high-fiber, plant-based diet: the
McDougall diet. The diet should be based around starches with the addition
of fruits and vegetables – there are no added vegetable oils. Sample foods
are: oatmeal, whole wheat pancakes or potatoes for breakfast. Lunch can be
soups, salads, and sandwiches. And dinner may be thought of in terms of
ethnic dishes, like Mexican burritos, Chinese Mu Shu vegetables, Thai
curried rice, or Italian whole grain pasta.
3) Ask them to exercise. Start at a comfortable level and gradually
build up. Exercise should be increased to the equivalent of at least a
half hour of walking a day.
4) Check their other risk factors for indications of serious disease,
such as cholesterol, triglycerides, and blood pressure. Then make diet and
lifestyle modifications to correct these (for example, fewer fruits and
juices with high triglycerides and cholesterol, and less salt with high
blood pressure).
5) Have them take appropriate medications only. For example, I
prescribe:
· Small doses of insulin for too much weight loss or if my patient
develops symptoms of diabetes, like too frequent urination or excessive
thirst.
· Cholesterol (and triglyceride) lowering medications in order to reach
ideal levels of 150 mg/dl, especially for patients at high risk for a
stroke or heart attack. (See my September 2002 and June 2003 Newsletters.)
· Blood pressure lowering medications, are sometimes indicated in
high-risk patients whose blood pressure remains at 160/100 mm Hg or
greater for months. (See my August 2002 Newsletter.)
A prescription of a low-fat diet and exercise can be taught by any
interested physician or dietitian. Most diabetics respond within days –
and with continued weight loss, most can be expected to stop all diabetic
medications – and regain lost health and appearance. The most difficult
task for people with diabetes is to break from tradition – the following
words may help. “The diet recommended by the American Diabetic Association
virtually guarantees all diabetics will remain diabetic,” claimed the
pioneer nutritionist, Nathan Pritikin, 30 years ago. His experiences from
treating thousands of people with this disease convinced him that type-2
diabetes is largely curable by following a healthy diet and moderate
exercise. Obviously the failure of modern diabetic management has been
known long before most diabetics developed their disease – yet nothing
changes for the better. Your only chance is to rebel against commonly
accepted advice. Don’t you think a revolt is long overdue based on the
poor results you have experienced so far?
References:
1) Narayan KM. Lifetime risk for diabetes mellitus in the United
States. JAMA 2003; 290: 1884-90.
2) Ludwig DS, Ebbeling CB. Type 2 diabetes mellitus in children:
primary care and public health considerations. JAMA. 2001 Sep
26;286(12):1427-30.
3) Joslin EP. Atheroscleriosis and diabetes. Ann Clin Med 1927;5:1061.
4) Hinsworth HP. Diet in the aetiology of diabetes. Proc R Soc Med
1949;42:323-6
5) West KM, Kalbfleisch JM,. Influence of nutritional factors on
prevalence of diabetes. Diabetes 1971; 20: 99-108.
6) Rao RH. The role of undernutrition in the pathogenesis of diabetes
mellitus. Diabetes Care 1984; 7: 595-601.
7) Lee ET, Welty TK, Cowan LD, Wang W, Rhoades DA, Devereux R, Go O,
Fabsitz R, Howard BV. Incidence of diabetes in American Indians of three
geographic areas: the Strong Heart Study. Diabetes Care. 2002
Jan;25(1):49-54.
8) McMurry MP . Changes in lipid and lipoprotein levels and body weight
in Tarahumara Indians after consumption of an affluent diet. N Engl J Med.
1991 Dec 12;325(24):1704-8.
9) Briceno I, Barriocanal LA, Papiha SS, Ashworth LA, Gomez A, Bernal
JE, Alberti KG, Walker M. Lack of diabetes in rural Colombian Amerindians.
Diabetes Care. 1996 Aug;19(8):900-1.
10) Foliaki S. Prevention and control of diabetes in Pacific people.
BMJ. 2003 Aug 23;327(7412):437-9.
11) Ring I. The health status of indigenous peoples and others. BMJ.
2003 Aug 23;327(7412):404-5.
12) Ko G. Rapid increase in the prevalence of undiagnosed diabetes and
impaired fasting glucose in asymptomatic Hong Kong Chinese. Diabetes Care.
1999 Oct;22(10):1751-2.
Mann JI. Diet and risk of coronary heart disease and type 2 diabetes.
Lancet. 2002 Sep 7;360(9335):783-9.
13) Fujimoto WY. The importance of insulin resistance in the
pathogenesis of type 2 diabetes mellitus. Am J Med. 2000 Apr 17;108 Suppl
6a:9S-14S.
14) Goldstein BJ. Insulin resistance as the core defect in type 2
diabetes mellitus. Am J Cardiol. 2002 Sep 5;90(5A):3G-10G.
15) UK Prospective Diabetes Study (UKPDS) Group. Intensive
blood-glucose control with sulphonylureas or insulin compared with
conventional treatment and risk of complications in patients with type 2
diabetes (UKPDS 33). Lancet. 1998;352:837-853.
16) DCCT Research Group. The effect of intensive treatment of diabetes
on the development and progression of long-term complications in insulin
dependent diabetes mellitus. N Engl J Med. 1993;329:977-986.
17) Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy
prevents the progression of diabetic microvascular complications in
Japanese patients with non-insulin-dependent diabetes mellitus: a
randomized prospective 6-year study. Diabetes Res Clin Pract.
1995;28:103-117
18) Engler RL, Yellon DM. Sulfonylurea KATP blockade in type II
diabetes and preconditioning in cardiovascular disease. Time for
reconsideration. Circulation. 1996 Nov 1;94(9):2297-301.
19) Garratt KN, Brady PA, Hassinger NL, Grill DE, Terzic A, Holmes DR
Jr. Sulfonylurea drugs increase early mortality in patients with diabetes
mellitus after direct angioplasty for acute myocardial infarction. J Am
Coll Cardiol. 1999 Jan;33(1):119-24.
20) Purnell JQ. Effect of excessive weight gain with intensive therapy
of type 1 diabetes on lipid levels and blood pressure: results from the
DCCT. Diabetes Control and Complications Trial. JAMA. 1998 Jul
8;280(2):140-6.
21) Colwell JA, Clark CM Jr. Forum Two: Unanswered research questions
about metabolic control in non-insulin-dependent diabetes mellitus. Ann
Intern Med. 1996 Jan 1;124(1 Pt 2):178-9.
22) Gustafsson I, Hildebrandt P, Seibaek M, Melchior T, Torp-Pedersen
C, Kober L, Kaiser-Nielsen P. Long-term prognosis of diabetic patients
with myocardial infarction: relation to antidiabetic treatment regimen.
The TRACE Study Group. Eur Heart J. 2000 Dec;21(23):1937-43.
23) McDougall J. McDougall’s Medicine – A Challenging Second Opinion.
New Century Publication 1985.
24) Kiehm TG, Anderson JW, Ward K. Beneficial effects of a high
carbohydrate, high fiber diet on hyperglycemic diabetic men. Am J Clin
Nutr. 1976 Aug;29(8):895-9.
25) Jenkins DJ, Kendall CW, Marchie A, Jenkins AL, Augustin LS, Ludwig
DS, Barnard ND, Anderson JW. Type 2 diabetes and the vegetarian diet. Am J
Clin Nutr. 2003 Sep;78(3 Suppl):610S-616S.
26) Nicholson AS, Sklar M, Barnard ND, Gore S, Sullivan R, Browning S.
Toward improved management of NIDDM: A randomized, controlled, pilot
intervention using a lowfat, vegetarian diet. Prev Med. 1999
Aug;29(2):87-91.
27) Raal FJ, Kalk WJ, Lawson M, Esser JD, Buys R, Fourie L, Panz VR.
Effect of moderate dietary protein restriction on the progression of overt
diabetic nephropathy: a 6-mo prospective study. Am J Clin Nutr. 1994
Oct;60(4):579-85.
28) Cupisti A. Vegetarian diet alternated with conventional low-protein
diet for patients with chronic renal failure. J Ren Nutr. 2002
Jan;12(1):32-7.
29) Van Eck W. The effect of a low fat diet on the serum lipids in
diabetes and its significance in diabetic retinopathy. Am J Med. 1959;
27:196-211.
30) Kempner W. Effect of the rice diet on diabetes mellitus associated
with vascular disease. Postgrad Med. 1958; 24:359-71.
31) Ornish D, Brown SE, Scherwitz LW, Billings JH, Armstrong WT, Ports
TA, McLanahan SM, Kirkeeide RL, Brand RJ, Gould KL. Can lifestyle changes
reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990
Jul 21;336(8708):129-33.
32) Segasothy M, Phillips PA. Vegetarian diet: panacea for modern
lifestyle diseases? QJM. 1999 Sep;92(9):531-44.
33) Fraser G. Ten years of life. Is it a matter of chance? Arch Intern
Med. 161:1645-52, 2001.
34) Key TJ, Davey GK, Appleby PN. Health benefits of a vegetarian diet.
Proc Nutr Soc. 1999 May;58(2):271-5.
35) Sabate J. The contribution of vegetarian diets to health and
disease: a paradigm shift? Am J Clin Nutr. 2003 Sep;78(3 Suppl):502S-507S.
36) Nicholas P. Hays; Raymond D. Starling; Xiaolan Liu; Dennis H.
Sullivan; Todd A. Trappe; James D. Fluckey; William J. Evans. Effects of
an Ad Libitum Low-Fat, High-Carbohydrate Diet on Body Weight, Body
Composition, and Fat Distribution in Older Men and Women: A Randomized
Controlled Trial. Arch Intern Med. 2004;164:210-217.
37) Jequier E, Bray GA. Low-fat diets are preferred. Am J Med. 2002 Dec
30;113 Suppl 9B:41S-46S.
38) Astrup A, Astrup A, Buemann B, Flint A, Raben A. Low-fat diets and
energy balance: how does the evidence stand in 2002? Proc Nutr Soc. 2002
May;61(2):299-309.
39) Wing R. Successful weight loss maintenance. Annu Rev Nutr.
2001;21:323-41.
40) Pinkney J. Prevention and cure of type 2 diabetes. BMJ. 2002 Aug
3;325(7358):232-3.
You may subscribe to this free McDougall Newsletter at http://www.drmcdougall.com
2004 John McDougall All Rights Reserved
Fair Use Notice: This document may contain copyrighted material whose
use has not been specifically authorized by the copyright owners.
We believe that this not-for-profit, educational
use on the Web constitutes a fair use of the copyrighted material (as
provided for in section 107 of the US Copyright Law). If you wish to use
this copyrighted material for purposes of your own that go beyond fair
use, you must obtain permission from the copyright owner.